 What is ECMO?
What is ECMO?
ECMO is a type of prolonged mechanical cardiopulmonary support that is usually delivered in the intensive care unit. ECMO is performed by clinicians with training and experience in its initiation, maintenance, and discontinuation.
How does it function?
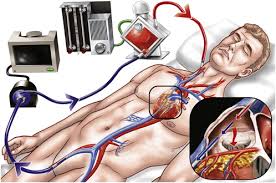
During ECMO, blood is drained from the native vascular system, circulated outside the body by a mechanical pump, and reinfused into the circulation. While outside the body, the blood passes through an oxygenator and heat exchanger. In the oxygenator, hemoglobin becomes fully saturated with oxygen, while carbon dioxide (CO2) is removed. Oxygenation is determined by flow rate, where elimination of CO2 can be controlled by adjusting the rate of countercurrent gas flow through the oxygenator.
What are the types?
ECMO can be venovenous (VV) or venoarterial (VA):
● During VV ECMO, blood is extracted from the vena cava or right atrium and returned to the right atrium. VV ECMO provides respiratory support, but the patient is dependent upon his or her own hemodynamics.
● During VA ECMO, blood is extracted from the right atrium and returned to the arterial system, bypassing the heart and lungs. VA ECMO provides both respiratory and hemodynamic support. The additional benefit of hemodynamic support comes with additional risks.
VV ECMO is used in patients with respiratory failure, while VA ECMO is used in patients with cardiac failure.
Who is given ECMO?
Patients with severe, but potentially reversible, acute respiratory or cardiac failure that is unresponsive to conventional management are evaluated for ECMO.
What is the procedure?
Once it has been determined that ECMO will be initiated, the patient is anticoagulated. Cannulae are then inserted and the patient is connected to the ECMO circuit. The blood flow is increased until respiratory and hemodynamic parameters are satisfactory. Once the initial respiratory and hemodynamic goals have been achieved, blood flow is maintained, ventilator support is minimized, and vasoactive drugs are decreased to minimal levels.
The patient’s readiness for weaning from ECMO should be evaluated frequently. Prior to discontinuing ECMO permanently, one or more trials should be performed during which the patient is off ECMO. Such trials give the clinician the opportunity to determine whether conventional supportive care is sufficient for the patient.
What are the complications?
Bleeding is the most common complication (30 to 40 percent) of ECMO. Thromboembolism and cannula complications are rare (<5 percent).
What are the contraindications?
The only absolute contraindication to ECMO is a pre-existing condition which is incompatible with recovery (severe neurologic injury, end stage malignancy). Relative contraindications include uncontrollable bleeding and very poor prognosis from the primary condition. Results in respiratory failure are better when ECMO is instituted within seven days of intubation.
What are the studies in cardiac arrest?
Venoarterial (VA) ECMO can provide acute support in cardiogenic shock or cardiac arrest in adults. Assuming that the brain function is normal or only minimally impaired.
ECMO is provided until the patient recovers or receives a long-term ventricular assist device as a bridge to cardiac transplantation. Observational studies and case series have reported survival rates of 20 to 50 percent among patients who received ECMO for cardiac arrest, severe cardiogenic shock, or failure to wean from cardiopulmonary bypass following cardiac surgery.
In two observational studies, ECMO performed for cardiac arrest was associated with increased survival compared to conventional cardiopulmonary resuscitation [Crit Care Med 2011; 39:1, Lancet 2008; 372:554.].
In a systematic review of adults with refractory out of hospital cardiac arrest, survival was 22 percent in the 833 patients who received ECMO during resuscitation and half of these had good neurological recovery